
The Deadly Gap: What New Active-Shooter Medical Research Means for You
A new analysis published in *JEMS* (the Journal of Emergency Medical Services) opens with a timeline that should stop every prepared citizen in their tracks. An officer makes entry. Twelve minutes later, the shooter is neutralized and the threat contained. But it isn't until the 24-minute mark that a medical team reaches a victim with a chest wound and a collapsing lung. By then the patient has gone nearly half an hour without being able to breathe, and dies moments later—even though the lifesaving procedure was performed the instant help arrived.
The author, Stephen P. Wood, calls this what it is: not a failure of medical knowledge, but a failure to put that knowledge to work in time. It's a sobering read, and while it's written for EMS professionals and agency leaders, the lessons land squarely on anyone who takes personal preparedness seriously.
Here's our summary of the key points—and what we think they mean for you.
The doctrine is good. The execution often isn't.
There is an established national standard for medical response during an active shooter event. It calls for trained providers to begin care in the “warm zone”—an area where the immediate threat has been suppressed but isn't fully cleared—within ten minutes of arriving near the wounded.
Wood's argument is not that the standard is wrong. It's that after-action reviews keep showing the same thing: those benchmarks frequently aren't met in real incidents. The gap isn't in the doctrine. It's in the institutional will, equipment, and culture needed to actually carry it out.
What's actually killing people may surprise you
This is the part of the article most relevant to how civilians think about trauma care.
Most “Stop the Bleed”-style training—rightly—emphasizes extremity bleeding and tourniquets, drawing heavily on military combat experience where blood loss from arms and legs was the leading preventable cause of death. But the research Wood cites shows that civilian mass shootings look different. The leading causes of potentially preventable death are chest and spinal injuries: tension pneumothorax, open (“sucking”) chest wounds, and airway compromise.
We have previously discussed this on our YouTube channel. The wound patterns in this mass murder events tend toward chest wounds.
That distinction matters because of timing. A tourniquet can be applied by almost anyone with a few minutes of training. But chest injuries follow an unforgiving clock—a tension pneumothorax can progress toward irreversible collapse in roughly 5 to 15 minutes, and airway problems even faster. These conditions demand recognition and intervention quickly, which is exactly why the delay described in that opening scenario is fatal.
The uncomfortable conclusion: even a perfectly executed 10-minute response may arrive too late for some of these injuries.
Two incidents, two outcomes
Wood contrasts two well-known events to show that the difference between life and death was implementation, not doctrine.
At the Pulse nightclub in 2016, the threat was contained in a bathroom while casualties lay in an area that met every definition of a warm zone. The local fire department had spent years developing a plan and had even purchased the protective equipment for exactly this situation. It was never deployed; EMS stayed blocks away. Analysis later estimated that around 16 casualties might have survived with basic care in the first ten minutes.

At the Route 91 festival in Las Vegas in 2017, the local fire department had outfitted every frontline unit with ballistic protection in advance. When the shooting stopped—with the scene still uncertain—crews moved into the warm zone under police escort rather than waiting for an all-clear. The federal after-action report credited that equipment and that decision directly with saving lives.
Same doctrine. Opposite results. The variable was preparation and the willingness to act.
The military lesson is about everyone, not just medics
The article also pushes back on the idea that the answer is simply “more medics.” The military's success in reducing preventable battlefield deaths came largely from training *every* service member in basic lifesaving care—not from relying on a handful of specialists. The lesson isn't “embed a professional everywhere.” It's that lifesaving capability has to be distributed to the people who are already there when someone is hurt.
Where this leaves the prepared citizen
We want to be careful and honest here, because that's how we approach everything.
This article is about professional and law-enforcement response. It is not an argument that civilians should be performing advanced procedures like needle decompression—Wood notes that even having officers trained to do it is considered controversial within the field.
But strip the scenario down and one fact remains: in the minutes between the moment someone is wounded and the moment trained help reaches them, the only care available is whatever the people already on scene can provide. The whole debate in this article exists because that gap is real, it is often long, and the injuries that fill it are frequently survivable with timely care.
That is the entire premise behind taking personal medical preparedness seriously. A few practical takeaways worth sitting with:
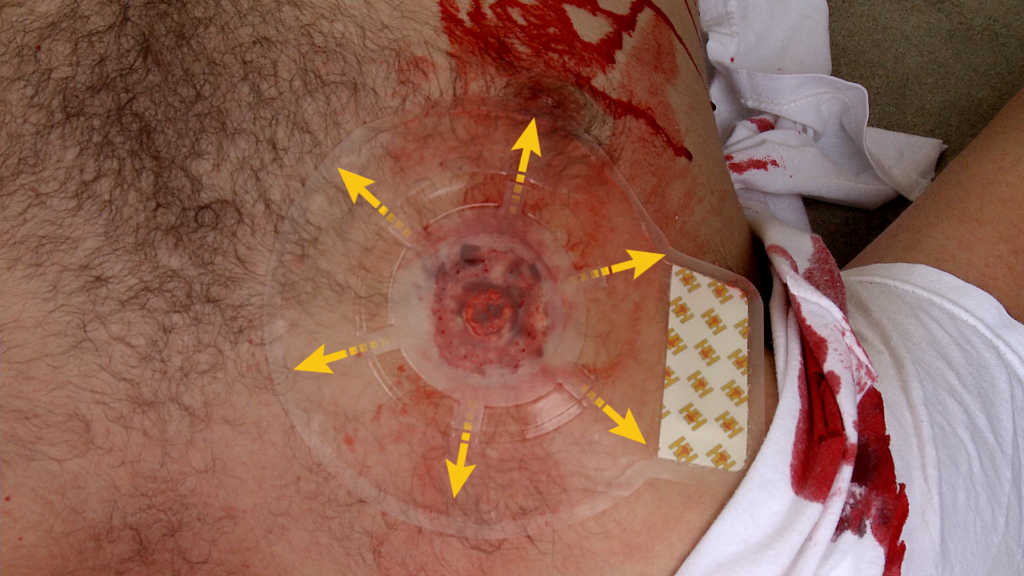
- Bleeding control is necessary but not the whole picture. Tourniquets and wound packing save lives, and you should know them cold. But the research is a clear reminder that chest trauma is a major killer in these events—which is why a complete kit includes chest seals and why understanding how to recognize and treat a chest wound belongs in your training, not just bleeding control.
- Skills and gear are a package deal. The Las Vegas responders didn't save lives because they had equipment; they saved lives because they had equipment and the training and willingness to use it. The same logic applies to you. A kit you don't know how to use is decoration.
- The clock is the enemy. The reason any of this matters is time. You can't shorten the response time of the professionals, but you can be the capable hands that are already there.
None of this is about replacing EMS, playing hero, or carrying gear for situations you'll almost certainly never face. It's about closing the most dangerous gap in any emergency—the one before help arrives—with real skills and a kit built from proven components.
—
The original article, “When Active Shooter Medical Doctrine Fails at the Point of Wounding” by Stephen P. Wood, DMSc, ACNP, is worth reading in full at JEMS.com.
Want to close the gap in your own preparedness? Subscribe to our YouTube channel for hands-on technique demonstrations, and sign up for our newsletter for training resources and educational content built for the armed citizen.